Eye Exams in Wilkes-Barre
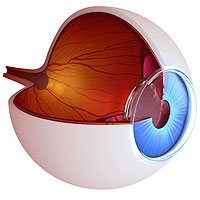
Your eyes are surprisingly complex and resilient – as well as very necessary. Many people take their eye health for granted. Your eyes aren’t something you think much of until there’s something wrong. Here at Eyecare Specialists, we strive to get patients thinking about their long-term eye health and ways they can prevent eye disease. This all starts with routine eye exams and general eye care.
What do eye exams prevent?
Eye examinations are performed for preventative and diagnostic purposes. While eye examination may not prevent all eye disease, they give your eye doctor the ability to diagnose eye diseases early on. Usually, an early diagnosis means the best treatment outcomes. Eye examinations prevent and diagnose eye diseases such as glaucoma, dry eye syndrome, cataracts, diabetic retinopathy, and refractive error.
What happens during an eye exam?
Regular eye examinations are the foundation of your eye health. They help with prevention and catching an eye disease early on for best treatment outcomes. But what actually happens during an eye exam?
Eye examinations are fairly quick, easy and painless. Your routine eye examination will include:
- Visual acuity tests. You will look at a projected eye chart to measure your visual acuity at distances. You may also look at a handheld chart to measure near vision.
- Color blindness test. You may need a screening to rule out color blindness. This may also alert your doctor to eye health issues that can cause color blindness.
- Cover test. This test allows your doctor to examine how well your eyes work together.
- Ocular motility test. Ocular motility refers to how well your eyes can follow a moving object. Problems with eye movement can cause eyestrain and can affect reading ability, among other things.
- Glaucoma test. During this test, your eye doctor will measure the pressure inside of your eye using a tonometer. Your eyes will be numbed using eye drops, and the tonometer pressed gently against the eye to get the reading.
- Pupil Dilation. In order to get a good look at the inside of your eye, your eye doctor will use dilating drops to enlarge the pupil. These drops can take 20 to 30 minutes to start working. After this, you will be sensitive to light and may have trouble focusing on objects up close. This will only last a couple of hours.
- Other Eye Tests. Depending on the results of these other screenings, your doctor may need to run more tests to rule out eye disease.
How often should I get an eye exam?
This depends on your current health and previous eye disease. For example, if you are diabetic, you will be asked to come back once a year. The same goes for people over the age of 50 or anyone with a previous diagnosis. If you are young and in good health, you may only be asked back every 2 to 3 years. Your eye doctor will let you know when you need to come back.
Searching for an eye doctor in Scranton or Wilkes-Barre that suits your needs? Look no further than Eyecare Specialists. We’re here to keep you and your family healthy and seeing their absolute best. Be sure to give us a call to set up your eye examination!